
Touch It
Feb 07, 2019
I spend a great deal of my time with patients trying to correct lots of misinformation or misunderstandings they get from many other sources, such as the media, the internet, and other clinicians. One subject I challenge a lot is when patients have been told that their pain is due to a part of their body being too stiff or too loose as discovered by a clinician expertly touching it.
I'm still astounded at the number of myths and misconceptions that still exist around touch and palpation within musculoskeletal therapy. I have discussed this before over the years here and here, but I feel I need to again as many therapists are still peddling some utter crap to patients about what they can diagnose by touch.
Crystal clear
However, before I begin let me make this crystal clear for all those who like to sling false dichotomies and straw men at me, I am not questioning the THERAPEUTIC benefits of touch here, although I do think this is an over-egged and over-exaggerated point as I don't think most touch done by therapists is that therapeutic often being poky, painful and uncomfortable than soothing, relaxing or caring.
I am also NOT saying that we should NOT touch our patients, in fact just the opposite. I actually advocate that all therapists take the time to thoroughly examine their patients, which includes palpation, as this is a basic, critical and essential part of all assessments. There is nothing worse than hearing a patient tell me that they last clinician they saw didn't even bother to look at the area that concerns them let alone touch it.
This lazy, sloppy, and downright dangerous approach to palpation is just as bad as those who make over the top, complex, ridiculous, nonsensical, and far fetched claims about it. Taking the time to examine a patient's painful area with palpation feeling for any swelling, heat, or gross deformity is a simple basic fundamental part of a good assessment.
Ridiculous!
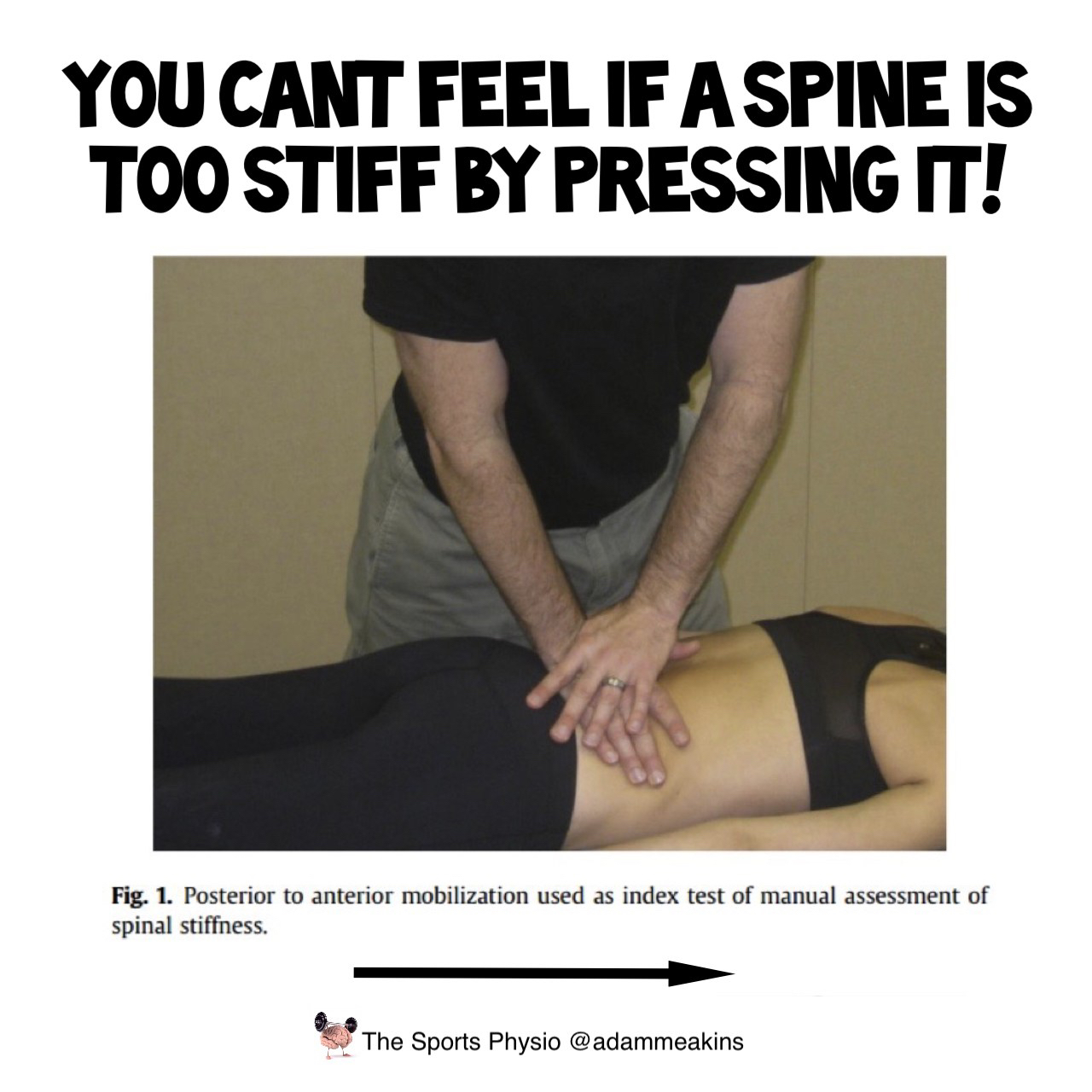
However, many therapists do take the notion of the skill of palpation to the realms of ridiculousness claiming that they can feel some downright crazy things. For example, many therapists think they can feel specific vertebra in spines that are too stiff, too loose, or not moving correctly when performing the common Maitland passive accessory movement tests or PAIVMs. However, there is a large body of evidence of many years, from many researchers that shows very little to no reliability or utility of these so-called diagnostic tests (ref, ref, ref, ref, ref, ref).
Also, many therapists still think they can feel the teeny tiny movements of the sacroiliac joint moving either too much or not enough under layers of thick muscle and dense ligaments, again despite this being refuted many, many times of the years (ref, ref, ref, ref).
Many therapists think they can feel knots and taut bands in muscles despite the evidence demonstrating, again and again, no reliability (ref, ref, ref, ref, ref). Some deluded individuals even think they can feel blockages in cerebrospinal fluids under the bones of the skull which defies any scientific plausibility or common sense (ref, ref).
And finally, there are also the shysters and crackpots who think they can feel blocked energy, distorted auras, and other mystical claptrap who need to be rounded up and catapulted into the sun.
Student days!
Now I can understand why many therapists think they can feel some of these things because its what they get taught from tutors who they trust and respect. I can remember as a student some 20 years ago now being taught to feel for stiff spines, wonky pelvises, and tight muscles using palpation. I was taught to push joints and soft tissues to feel if they moved too little, or too much, feel for overactivity, tightness, and spasm.
Yet despite hours and hours of practice and seeing many others all around me saying they could feel this stuff, I just couldn't feel jack shit. I was told that I had to keep practising and then I would be able to feel the things my peers and tutors could. So I did, for years and years, but I still couldn't feel diddly squat, and I still can't feel jack shit 20 years later.

The first issue I had was trying to decide what is too stiff or too loose. For me to be able to identify what's abnormal I first need to establish what's normal.
However, during my student training when I was pressing, poking, prodding my mates and other normal pain-free fully functional people I found them to all be variable in feelings of stiffness, tightness, and lumpiness.
With this wide variation in texture and feel in so called normal people (if you can class physio students as 'normal'), how the hell am I supposed to decide if someone in pain is too stiff or too lumpy?
Another problem I found was any feelings of stiffness were highly dependant on the force I applied to an individual. When I pressed lighter they felt stiffer, when I pressed heavier they felt looser.
This variability in force meant I could change the feel of something being too stiff or not. And plenty of research has demonstrated huge variation in the forces that therapists apply with these tests meaning any interpretations of stiffness will also be hugely variable (ref, ref, ref, ref).
The final issue I had with diagnostic palpation tests was trying to feel what I was supposed to feel. For example, I had difficulty in determining if a lump felt in a muscle was an abnormality or a normal anatomical structure. I also had issues with trying to interpret what I was feeling was actually the structure I was supposed to be palpating and not the other tissues above it.
I even had difficulty finding something as simple as a specific spinal level, and I still do. For example, I would be thinking I am palpating a C6 or L4 vertebra when in fact I could be 1 or 2 levels out. And before you think I am an idiot here it's not just me that can't reliably find them, many, many other experienced and skilled clinicians have been shown to be very poor at identifying specific bony structures and vertebral levels (ref, ref, ref).
Ignorance, ego, and fear
So why is it that despite these issues and decades of research demonstrating poor reliability of diagnostic palpation tests do so many therapists continue to use them, and are adamant that they can feel things that evidence says they cant?
Well, I think its a combination of ignorance, ego, and fear. Most therapists who continue to use these palpation tests simply haven't kept up with the research and are unaware of these reliability issues, and more importantly that these tests are not correlated with patients pain or problems.
Those therapists that are aware, or have read this research, yet still continue to use and teach these diagnostic palpation tests usually do so due to cognitive dissonance. Usually, their ego refuses to let them abandon something that they have spent so long working on to perfect, and which has involved investing a lot of time, energy, and money to learn.
And believe it or not, I do empathise a lot with these therapists, as someone who has spent many years of my life and thousands of my hard-earned sheckles on training in palpation and manual therapy seeking to become a better physio, I also feel annoyed, frustrated, and cheated, but I got over it and moved on.

The final reason I think many therapists refuse to abandon these unreliable and unevidenced diagnostic palpation tests is fear. A fear of inadequacy. Many therapists are just not comfortable or confident with themselves or their position within healthcare, often feeling inferior and subservient to our medical and surgical colleagues. So to inflate their position and give them more confidence they often claim to be able to do highly specialised and skilled things which others can not.
But therapists don't need superhuman powers of palpation to be respected. Therapists don't need Jedi manual therapy skills or belief in mysterious, mystical forces to be confident in what they do. If more therapists just had more confidence in the simple basic things such as getting people in pain and disability back to the things they want to do, with advice, reassurance, encouragement, activity, and of course exercise, then I think we would be respected even more by our colleagues.
Universities need to change!
I want to finish by asking why, in 2019, are so many physio students still being taught these unreliable palpation tests. Why are so many universities still teaching students spinal PIAVMs, PAMs, SIJ palpation, and trigger points assessments? Why are students still being asked to feel for things they will never be able to feel. Why are students being made to feel inadequate or unskilled just like I was 20 years ago?
I think one of the many reasons why this kind of bull shit still persists... the very strong financial incentives. All these palpation/manual therapy courses feed of therapist fears, ignorance and inadequacy issues by promising them better skills in palpation for a lot of money and reward those teaching them very well.
But here's the thing, these postgrad courses would soon be redundant and obsolete if students were taught in university about the issues with these tests, and shown the research about diagnostic palpation, and not be made to feel inadequate or unskilled so that they keep searching and practising on fake shitty courses in an attempt to feel like good therapists.
So I will sign off by once again reiterating that these diagnostic joint motion palpation and muscle trigger point tests are unreliable and not needed to help patients or to be a good therapist. But, please do take the time to fully examine and palpate your patients, just remember to use your common sense, and the evidence, to help inform you what you can and can not feel in a patient.
As always thanks for reading
Adam
Stay connected with new blogs and updates!
Join my mailing list to receive the latest blogs and updates.
Don't worry, your information will not be shared.
I hate SPAM, so I promise I will never sell your information to any third party trying to sell you laser guided acupuncture needles or some other BS.
